Arterial Blood gas Analysis(ABG)
Protocols
Reference ranges
- pH: 7.35 – 7.45
- PaCO2: 4.7 – 6.0 kPa || 35.2 – 45 mmHg
- PaO2: 11 – 13 kPa || 82.5 – 97.5 mmHg
- HCO3–: 22 – 26 mEq/L
- Base excess (BE): -2 to +2 mmol/L
Oxygenation(PaO2) :
Your first question when looking at the ABG should be “Is this patient hypoxic?” as hypoxia is the most immediate threat to life.
PaO2 should be >10 kPa (75mmHg) when oxygenating on room air in a healthy patient.
If the patient is receiving oxygen therapy their PaO2 should be approximately 10kPa less than the % inspired
concentration FiO2 (so a patient on 40% oxygen would be expected to have a PaO2 of approximately 30kPa /225mmHg).
Oxygen delivery devices and flow rates:
A common question is “What percentage of oxygen does this device deliver at a given flow rate?”. Below is a quick reference guide,
providing some approximate values for the various oxygen delivery devices and flow rates you’ll come across in practice.
Nasal cannulae
As with all oxygen delivery devices, there is a significant amount of variability depending on the patient’s breathing rate, depth and how
well the oxygen delivery device is fitted. Below are some guides to various oxygen flow rates and the approximate percentage of oxygen delivered:
1L / min – 24%
- 2L/ min – 28%
- 3L/ min – 32%
- 4L / min – 36%
Simple face mask
The oxygen delivery of simple face masks is highly variable depending upon oxygen flow rate, the quality of the mask fit, the
patient’s respiratory rate and their tidal volume. Simple face masks can deliver a maximum FiO2 of approximately 40%-60% at a
flow rate of 15L/min. These masks should not be used with flow rates less than 5L/min.
Reservoir mask (also known as a non-rebreather mask)
Reservoir masks deliver oxygen at concentrations between 60% and 90% when used at a flow rate of 10–15 l/min.
The concentration is not accurate and will depend on the flow of oxygen as well as the patient’s breathing pattern.
These masks are most suitable for trauma and emergency use where carbon dioxide retention is unlikely.
Venturi masks
A Venturi mask will give an accurate concentration of oxygen to the patient regardless of the oxygen flow rate (the minimum suggested
flow rate is written on each). Venturi masks are available in the following concentrations: 24%, 28%, 35%, 40% and 60%.
They are suitable for all patients needing a known concentration of oxygen, but 24% and 28% Venturi masks are particularly
suited to those at risk of carbon dioxide retention (e.g. patients with chronic obstructive pulmonary disease).
Hypoxaemia
If PaO2 is <10 kPa (75mmHg) on air, a patient is considered hypoxaemic.
If PaO2 is <8 kPa (60mmHg) on air, a patient is considered severely hypoxaemic and in respiratory failure.
Type 1 & 2 respiratory failure:
Type 1 respiratory failure involves hypoxaemia (PaO2 <8 kPa / 60mmHg) with normocapnia (PaCO2 <6.0 kPa / 45mmHg).
Type 2 respiratory failure involves hypoxaemia (PaO2 <8 kPa / 60mmHg) with hypercapnia (PaCO2 >6.0 kPa / 45mmHg).

Type 1 respiratory failure
Type 1 respiratory failure involves hypoxaemia (PaO2 <8 kPa /60mmHg) with normocapnia (PaCO2 <6.0 kPa / 45mmHg).
It occurs as a result of ventilation/perfusion (V/Q) mismatch; the volume of air flowing in and out of the lungs is not matched with the
flow of blood to the lung tissue. As a result of the VQ mismatch, PaO2 falls and PaCO2 rises. The rise in PaCO2 rapidly triggers an increase in
a patient’s overall alveolar ventilation, which corrects the PaCO2 but not the PaO2 due to the different shape of the CO2 and
O2 dissociation curves. The end result is hypoxaemia (PaO2 < 8 kPa /60mmHg) with normocapnia (PaCO2 < 6.0 kPa / 45mmHg).
Examples of VQ mismatch include:
- Reduced ventilation and normal perfusion (e.g. pulmonary oedema, bronchoconstriction)
- Reduced perfusion with normal ventilation (e.g. pulmonary embolism)
Type 2 respiratory failure
Type 2 respiratory failure involves hypoxaemia (PaO2 is <8 kPa / 60mmHg) with hypercapnia (PaCO2 >6.0 kPa / 45mmHg).
It occurs as a result of alveolar hypoventilation, which prevents the patient from being able to
adequately oxygenate and eliminate CO2 from their blood.
Hypoventilation can occur for a number of reasons including:
- Increased resistance as a result of airway obstruction (e.g. COPD).
- Reduced compliance of the lung tissue/chest wall (e.g. pneumonia, rib fractures, obesity).
- Reduced strength of the respiratory muscles (e.g. Guillain-Barré, motor neurone disease).
- Drugs acting on the respiratory centre reducing overall ventilation (e.g. opiates).
Seemingly small abnormalities in pH have very significant and wide-spanning effects on the physiology of
the human body. Therefore, paying close attention to pH abnormalities is essential.
So we need to ask ourselves, is the pH normal, acidotic or alkalotic?
- Acidotic: pH <7.35
- Normal: pH 7.35 – 7.45
- Alkalotic: pH >7.45

pH scale
We need to consider the driving force behind the change in pH. Broadly speaking the causes can be either metabolic or respiratory.
The changes in pH are caused by an imbalance in the CO2 (respiratory) or HCO3– (metabolic). These work as buffers to keep
the pH within a set range and when there is an abnormality in either of these the pH will be outside of the normal range.
As a result, when an ABG demonstrates alkalosis or acidosis you need to then begin considering what is driving this
abnormality by moving through the next few steps of this guide.
PaO2 :
At this point, prior to assessing the CO2, you already know the pH and the PaO2. So for example, you may know your patient’s pH is
abnormal but you don’t yet know the underlying cause. It could be caused by the respiratory system (abnormal level of CO2) or
it could be metabolically driven (abnormal level of HCO3-).
Looking at the level of CO2 quickly helps rule in or out the respiratory system as the cause for the derangement in pH.
| pH | CO2 | HCO3– | |
| Respiratory acidosis | ↓ | ↑ | Normal |
| Respiratory alkalosis | ↑ | ↓ | Normal |
| Respiratory acidosis with metabolic compensation | ↓ / ↔ | ↑ | ↑ |
| Respiratory alkalosis with metabolic compensation | ↑ / ↔ | ↓ | ↓ |
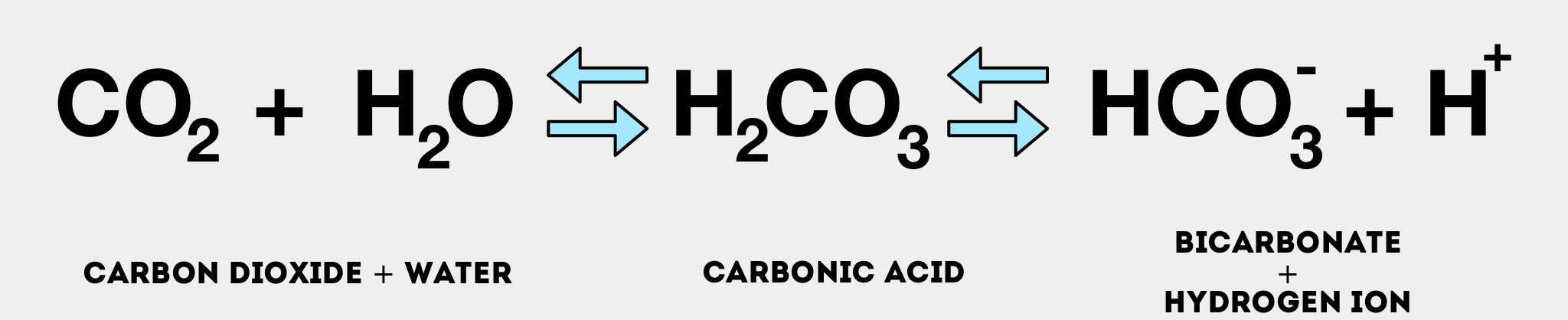
Underlying Biochemistry:
CO2 binds with H2O and forms carbonic acid (H2CO3) which will decrease pH. When a patient is retaining CO2 the
blood will, therefore, become more acidic from the increased concentration of carbonic acid. When a patient is ‘blowing
off’ CO2 there is less of it in the system and, as a result, the patient’s blood will become less acidotic and more alkalotic.
The idea of ‘compensation’ is that the body can try and adjust other buffers to keep the pH within the normal range.
If the cause of the pH imbalance is from the respiratory system, the body can adjust the HCO3– to counterbalance
the pH abnormality bringing it closer to the normal range. This works the other way around as well; if the
cause of a pH imbalance is metabolic, the respiratory system can try and compensate by either retaining
or blowing off CO2 to counterbalance the metabolic problem (via increasing or decreasing alveolar ventilation).
So we need to ask ourselves:
- Is the CO2 normal or abnormal?
- If abnormal, does this abnormality fit with the current pH (e.g. if the CO2 is high, it would make sense that
- the pH was low, suggesting this was more likely a respiratory acidosis)?
- If the abnormality in CO2 doesn’t make sense as the cause of the pH abnormality (e.g. normal or ↓ CO2 and ↓ pH),
- it would suggest that the underlying cause for the pH abnormality is metabolic.
HCO3– :
We now know the pH and whether the underlying problem is metabolic or respiratory in
nature from the CO2 level.
Piecing this information together with the HCO3– we can complete the picture:
- HCO3– is a base, which helps mop up acids (H+ ions).
- So when HCO3– is raised the pH is increased as there are less free H+ ions (alkalosis).
- When HCO3– is low the pH is decreased as there are more free H+ ions (acidosis).
So we need to ask ourselves:
- Is the HCO3– normal or abnormal?
- If abnormal, does this abnormality fit with the current pH (e.g. ↓HCO3– and acidosis)?
- If the abnormality doesn’t make sense as the cause for the deranged pH, it suggests the cause is more likely
- respiratory (which you should have already known from your assessment of CO2).
| pH | HCO3– | CO2 | |
| Metabolic acidosis | ↓ | ↓ | Normal |
| Metabolic alkalosis | ↑ | ↑ | Normal |
| Metabolic acidosis with respiratory compensation | ↓ | ↓ | ↓ |
| Metabolic alkalosis with respiratory compensation | ↑ | ↑ | ↑ |
You may note that in each of these tables HCO3– and CO2 are both included, as it is important to look at each in the context of the other.
Base Excess:
The base excess is another surrogate marker of metabolic acidosis or alkalosis:
1.A high base excess (> +2mmol/L) indicates that there is a higher than normal amount of HCO3– in the blood,
which may be due to a primary metabolic alkalosis or a compensated respiratory acidosis
2.A low base excess (< -2mmol/L) indicates that there is a lower than normal amount of HCO3– in the blood,
suggesting either a primary metabolic acidosis or a compensated respiratory alkalosis.

Compensation:
Compensation has been touched on already in the above sections, to clarify we have made it simple below:
1.Respiratory acidosis/alkalosis (changes in CO2) can be metabolically compensated by increasing or
decreasing the levels of HCO3– in an attempt to move the pH closer to the normal range.
2.Metabolic acidosis/alkalosis (changes in HCO3-) can be compensated by the respiratory
system retaining or blowing off CO2 in an attempt to move the pH closer to the normal range.

Role of compensation:
Respiratory compensation for a metabolic disorder can occur quickly by either increasing or decreasing
alveolar ventilation to blow off more CO2 (↑ pH) or retain more CO2 (↓ pH).
Metabolic compensation for a respiratory disorder, however, takes at least a few days to occur as it requires the
kidneys to either reduce HCO3– production (to decrease pH) or increase HCO3– production (to increase pH).
As a result, if you see evidence of metabolic compensation for a respiratory disorder (e.g. increased HCO3-/base excess
in a patient with COPD and CO2 retention) you can assume that the respiratory derangement has been ongoing for at least a few days, if not more.
It’s important to note that ‘over-compensation’ should never occur and, therefore, if you see something that resembles
this you should consider other pathologies driving the change (e.g. a mixed acid/base disorder).
mixed acidosis or alkalosis:
It’s worth mentioning that it is possible to have a mixed acidosis or alkalosis
(e.g. respiratory and metabolic acidosis/respiratory and metabolic alkalosis).
In these circumstances, the CO2 and HCO3– will be moving in opposite directions
(e.g. ↑ CO2 ↓ HCO3– in mixed respiratory and metabolic acidosis).
Treatment is directed towards correcting each primary acid-base disturbance.
You can see some causes of mixed acidosis and alkalosis below.

mixed respiratory and metabolic acidosis:
A mixed respiratory and metabolic acidosis would have the following characteristics on an ABG:
- ↓ pH
- ↑CO2
- ↓HCO3–
Causes of mixed respiratory and metabolic acidosis include:
- Cardiac arrest
- Multi-organ failure
mixed respiratory and metabolic alkalosis:
mixed respiratory and metabolic alkalosis would have the following characteristics on an ABG:
- ↑ pH
- ↓ CO2
- ↑ HCO3–
Causes of mixed respiratory and metabolic alkalosis:
- Liver cirrhosis in addition to diuretic use
- Hyperemesis gravidarum
- Excessive ventilation in COPD
Acid/Base Disturbance causes:
So far we have discussed how to determine what the acid-base disturbance is, once we have this established
we need to consider the underlying pathology that is driving this disturbance
Respiratory Acidosis:
Respiratory acidosis is caused by inadequate alveolar ventilation leading to CO2 retention.
A respiratory acidosis would have the following characteristics on an ABG:
- ↓ pH
- ↑ CO2
Causes of respiratory acidosis include:
- Respiratory depression (e.g. opiates)
- Guillain-Barre: paralysis leads to an inability to adequately ventilate
- Asthma
- Chronic obstructive pulmonary disease (COPD)
- Iatrogenic (incorrect mechanical ventilation settings)
Respiratory Alkalosis:
Respiratory alkalosis is caused by excessive alveolar ventilation (hyperventilation) resulting in more
CO2 than normal being exhaled. As a result, PaCO2 is reduced and pH increases causing alkalosis.
A respiratory alkalosis would have the following characteristics on an ABG:
- ↑ pH
- ↓ CO2
Causes of respiratory alkalosis include: ³
- Anxiety (i.e. panic attack)
- Pain: causing an increased respiratory rate.
- Hypoxia: resulting in increased alveolar ventilation in an attempt to compensate.
- Pulmonary embolism
- Pneumothorax
- Iatrogenic (e.g. excessive mechanical ventilation)
Metabolic acidosis:
Metabolic acidosis can occur as a result of either:
- Increased acid production or acid ingestion.
- Decreased acid excretion or increased rate of gastrointestinal and renal HCO3– loss.
A metabolic acidosis would have the following characteristics on an ABG:
- ↓ pH
- ↓ HCO3-
- ↓ BE
Anion gap :
Blood plasma is an aqueous solution containing a variety of chemical species, some of which have a net electrical charge
as a result of the dissociation of salts and acids in the aqueous medium. Species that have a net positive charge are called
cations (e.g. Na+, K+)and those with a net negative charge are called anions (chloride & HCO3–).
The anion gap is an artificial measure that is calculated by subtracting the total number of anions (chloride & HCO3–) from
the total number of cations (Na+). There are lots of other anions and cations, however, those shown in brackets have the most
significant influence, which is why other cations (e.g. K+) and anions (e.g. albumin, phosphate) are not used in the calculation of the anion gap.
Anion gap formula: Na+ – (Cl– + HCO3–)
The anion gap (AG) is a derived variable primarily used for the evaluation of metabolic acidosis to determine
the presence of unmeasured anions (e.g. albumin is the main unmeasured anion). The normal anion gap
varies with different assays but is typically between 4 to 12 mmol/L.
Causes of a high anion gap metabolic acidosis (typically relate to increased production/ingestion or
reduced excretion of H+ by the kidneys):
- Diabetic ketoacidosis
- Lactic acidosis
- Aspirin overdose
- Renal failure
Causes of a normal anion gap metabolic acidosis (typically due to loss of bicarbonate which is
subsequently replaced by chloride in the plasma, resulting in a stable overall anion concentration):
- Gastrointestinal loss of HCO3– (e.g. diarrhoea, ileostomy, proximal colostomy)
- Renal tubular disease
- Addison’s disease
Vignette
A 17-year-old patient presents to A&E complaining of a tight feeling in their chest, shortness of breath and some tingling in their fingers and around their mouth. They have no significant past medical history and are not on any regular medication. An ABG is performed on the patient (who is not currently receiving any oxygen therapy).
An ABG is performed and reveals the following:
- PaO2: 14 (11 – 13 kPa) || 105 mmHg (82.5 – 97.5 mmHg)
- pH: 7.49 (7.35 – 7.45)
- PaCO2: 3.6 (4.7 – 6.0 kPa) || 27 mmHg (35.2 – 45 mmHg)
- HCO3–: 24 (22 – 26 mEq/L)
Answer:
Oxygenation (PaO2)
A PaO2 of 14 on room air is at the upper limit of normal, so the patient is not hypoxic.
pH
A pH of 7.49 is higher than normal and therefore the patient is alkalotic.
The next step is to figure out whether the respiratory system is contributing the alkalosis (e.g. ↓ CO2).
PaCO2
The CO2 is low, which would be in keeping with an alkalosis, so we now know the respiratory system is
definitely contributing to the alkalosis, if not the entire cause of it.
The next step is to look at the HCO3– and see if it is also contributing to the alkalosis.
HCO3–
HCO3– is normal, ruling out a mixed respiratory and metabolic alkalosis, leaving us with an isolated respiratory alkalosis.
Compensation
There is no evidence of metabolic compensation of the respiratory alkalosis (which would involve a lowered HCO3-)
suggesting that this derangement is relatively acute (as metabolic compensation takes a few days to develop).
Interpretation
Respiratory alkalosis with no metabolic compensation.
The underlying cause of respiratory alkalosis, in this case, is a panic attack, with hyperventilation in addition
to peripheral and peri-oral tingling being classical presenting features.